 GlucoSpike AI
GlucoSpike AI
The 20-Year Study That Should Change How You Think About Prediabetes
3,234 people. 20 years. Lifestyle change: 21% fewer chronic diseases. Metformin: no difference from placebo. The data is in.

Every few months, a new study gets written up with a headline along the lines of 'This Drug Could Slow Aging.' Metformin has been the subject of a few of those. It's the most prescribed diabetes medication in the world, it's cheap, it's been around since the 1950s, and in recent years it became a darling of the biohacking crowd because of animal studies suggesting it might extend lifespan.
So here's a question worth asking: if you have prediabetes, and someone offers you metformin as a shortcut to better metabolic health, should you take it?
A study published in JAMA in June 2026 provides one of the most definitive answers we've had to that question. And the answer is not what the biohacking world wants to hear.
The study
The research draws from the Diabetes Prevention Program (DPP), one of the most important metabolic health trials ever conducted. Starting in 1996, researchers at 27 sites across the United States enrolled 3,234 adults who were at high risk for type 2 diabetes and followed them through 2021. That's 25 years of data.
In the original trial, participants were randomly assigned to one of three groups: an intensive lifestyle intervention, metformin (850mg twice daily), or a placebo. The lifestyle group was coached on reducing dietary fat, achieving at least 150 minutes of physical activity per week, and losing at least 7% of their body weight through 16 individual sessions followed by monthly check-ins.
This new JAMA analysis linked those participants' records to Medicare claims data and asked a bigger question: over 20 years, did either intervention protect people from developing multiple chronic conditions — not just diabetes, but the full cluster of diseases that come with metabolic dysfunction as people age?
What they found
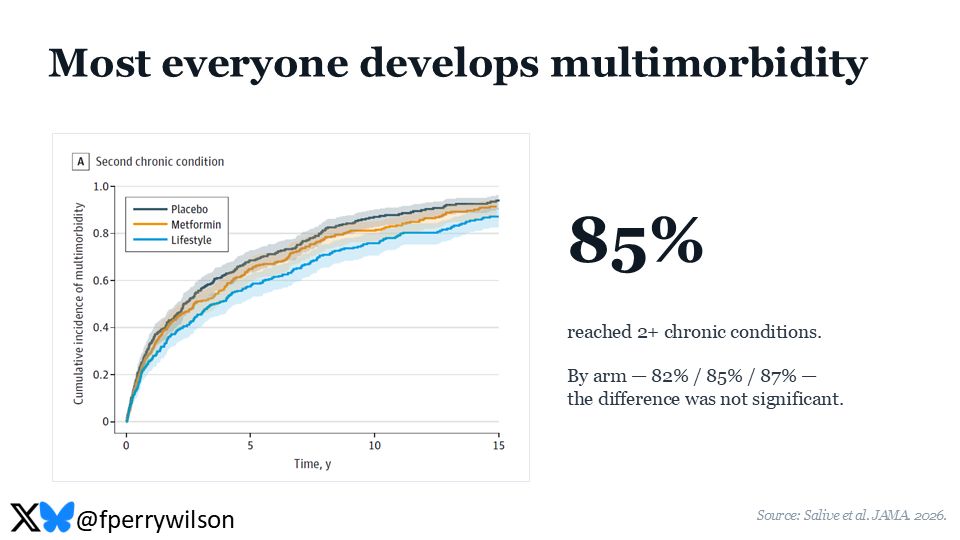
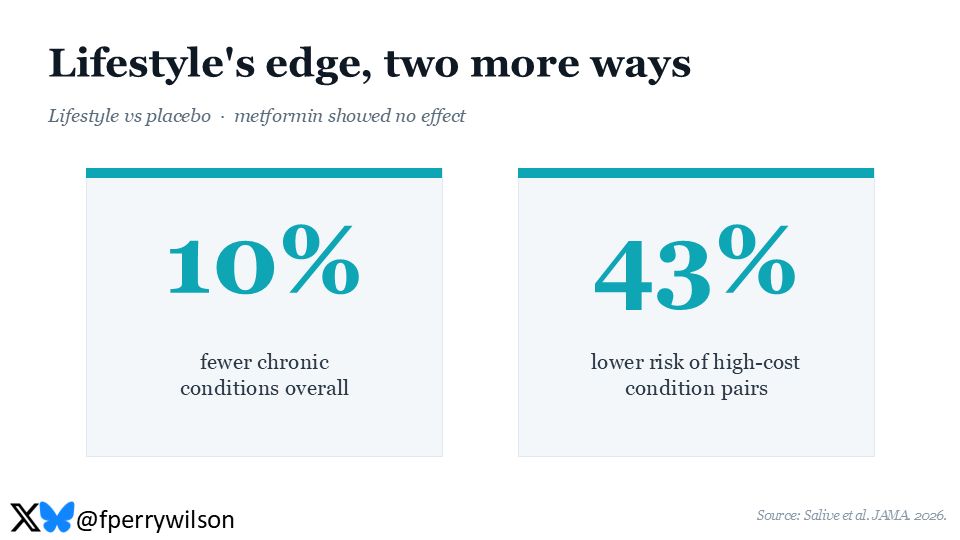
The lifestyle group had a 21% lower risk of developing multimorbidity — defined as two or more chronic conditions — compared to the placebo group. That protective effect held even when researchers accounted for diabetes onset itself, meaning the lifestyle changes were doing something broader than just preventing blood sugar problems.
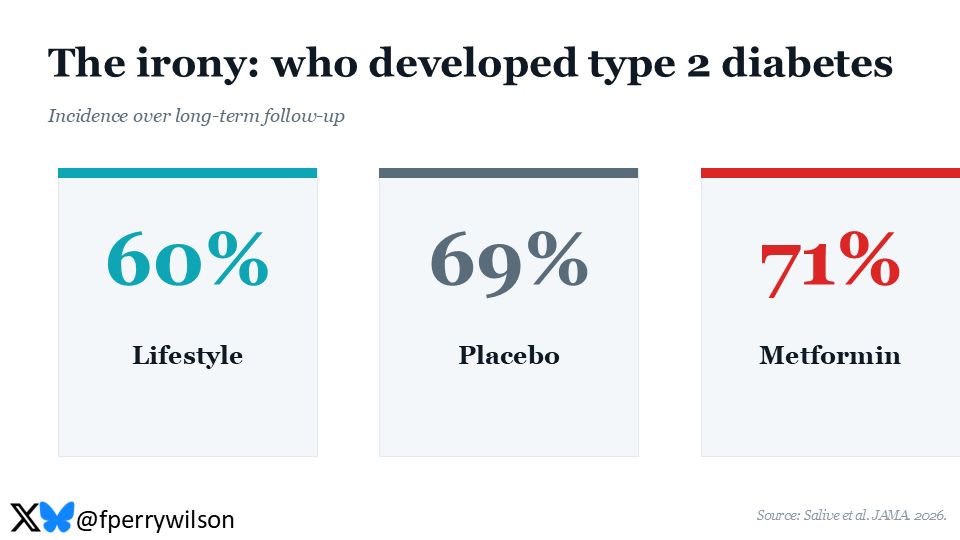
The metformin group showed no statistically significant reduction in multimorbidity compared to placebo.
Let that sit for a second. A medication that millions of people with prediabetes take — and that longevity enthusiasts are actively experimenting with — did not meaningfully reduce the long-term disease burden in people who had prediabetes. Consistent, structured lifestyle change did.
The 20-year tail of what you do today
The most important thing about this study is the timeframe. The lifestyle intervention happened between 1996 and 1999. People were coached for about three years. And yet the benefits were still detectable over 20 years later, measured through Medicare claims.
This is sometimes called a 'legacy effect' in metabolic research — early behavior changes that create a kind of biological memory that continues to confer protection even when active intervention ends. It's been documented with diabetes prevention before, but this is the first major analysis to show it extends to multimorbidity.
The study's lead author, Marcel Salive of the National Institute on Aging, noted that lifestyle modification, when it's safe and cost-effective, may help reduce both health burden and healthcare spending for people at risk of diabetes — particularly as they age into Medicare.
What 'multimorbidity' actually means
The study tracked 15 chronic conditions drawn from Medicare's Chronic Condition Warehouse. This isn't a narrow list. We're talking about heart disease, hypertension, stroke, kidney disease, depression, osteoporosis, Alzheimer's, COPD, and more.
Most older adults eventually accumulate several of these conditions simultaneously. That's the norm, not the exception. What the DPP study shows is that lifestyle intervention made during midlife — specifically targeted at metabolic health — may delay or prevent that accumulation. Preventing one condition isn't the goal. Preventing the pileup is.
An editorial accompanying the JAMA paper put it plainly: modest weight loss through healthier nutrition and increased physical activity remains a cornerstone for preserving quality of life and potentially promoting healthy longevity in this population.
Why this matters more than the biohacking narrative
There's a certain appeal to the idea that a pill can solve a metabolic problem. Metformin is inexpensive, generally well-tolerated, and feels like a way to hedge your bets without changing how you eat or how you move.
The 20-year DPP data suggests that's not how metabolism works. The people who reduced dietary fat, moved their bodies 150 minutes a week, and lost modest amounts of weight showed up in their Medicare data two decades later with meaningfully fewer chronic conditions. There's no equivalent signal for metformin on that outcome.
That's not to say metformin has no value — it does improve glucose control, and for people who have already progressed to type 2 diabetes, it remains a first-line medication. But for someone managing prediabetes or insulin resistance and hoping to avoid the cascade of chronic conditions that often follows, the evidence increasingly points in one direction: what you eat and how you move is doing work that no drug has replicated at scale.
The meal-level translation
The DPP lifestyle intervention was not complex. It didn't require a low-carb diet or intermittent fasting. The targets were: reduce dietary fat, move more, lose around 7% of body weight. What made it work was consistency over time.
At a practical level, this translates to hundreds of individual meal decisions. Not all at once, and not perfectly — but cumulatively, those decisions compound. A meal that avoids a sharp glucose spike reduces the load on your insulin system that day. Do that consistently over months and years and it adds up to a different metabolic trajectory.
The people in the lifestyle group weren't eating perfectly. They were eating better, more consistently, with support. The support structure mattered — which is why the program included regular individual sessions and monthly follow-ups, not just a handout with dietary advice.
What this means if you have prediabetes or insulin resistance right now
The DPP participants were in their early 50s on average. Many people reading this are in that window — the window where the habits you build now will show up in your health data 10 to 20 years from now.
The study doesn't say you need to be perfect. It says you need to be consistent. The intervention was modest by the standards of what people put themselves through online — no extreme protocols, no expensive supplements, just structured movement, better food choices, and some weight loss maintained over time.
The harder question is: how do you actually sustain that? The DPP had coaches and sessions and monthly check-ins. Most people don't have that. What they have is a phone, and the ability to start noticing what their meals are doing to them.
That's actually what GlucoSpike AI is built for — logging meals, scoring their likely glucose impact, and surfacing the patterns that repeat. Not a replacement for a doctor. Not a prescription. Just a way to turn your daily eating into data you can actually see and act on.
That awareness — knowing which meals cause energy crashes, which ones leave you feeling clear and stable, which patterns repeat — is where the behavior change actually begins. Not from a 20-page meal plan, but from recognizing your patterns and acting on them, meal by meal.
The JAMA data gives you the 20-year picture. What you choose to eat this week is one frame of it.
"Sugar-free" doesn't mean spike-free. Scan it and know.
The GlucoSpike app includes a free barcode scanner — point your camera at any packaged product and get an instant GS Score showing how it will hit your blood sugar, plus what to grab instead. 4M+ products, 150+ countries, free forever.


Scanner free forever · No credit card · See how it works →